
|
Prevalence |
|
Williams syndrome (WS) has historically been estimated to occur in roughly 1 in every 20,000 live births. However, more recent epidemiological studies have placed the occurrence rate at closer to 1 in every 7,500 live births, a significantly larger prevalence (Stromme, Bjornstad & Ramstad, 2002).
WS affects 1 in 10,000 people worldwide (Grimm & Wesselhoeft, 1980) – an estimated 20,000 to 30,000 people in the United States (Williams-syndrome.org, 2015) . As an increasing body of evidence suggests that Williams syndrome is more common than originally noted (approximately 6% of all genetic cases of developmental disability), researchers have begun to theorize past under-diagnosis of the disorder. One theorized reason for the increase in epidemiological estimates is that there exists a substantial minority of individuals with the genetic markers of Williams syndrome who lack the characteristic facial features or the diminished IQ considered to be diagnostic of the disorder, who often are not immediately recognized as people with the syndrome (Martens, Wilson & Reutens, 2008). Williams Syndrome occurs sporadically and spontaneously and is found equally in all ethnicities, races, socioeconomic backgrounds and genders. |
|

|
Early Warning Signs |
|
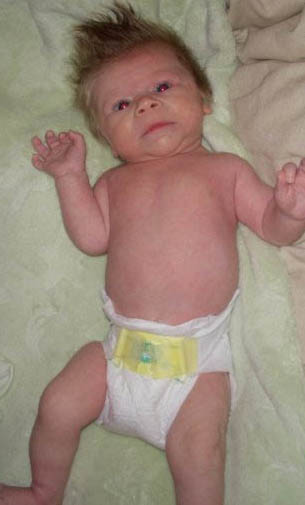
The condition is not always apparent when the child is born, therefore many children who have Williams Syndrome are often not diagnosed right away. The early warning signs or developing symptoms that may be apparent to a greater or lesser degree, include: facial dysmorphies characteristic of the syndrome, including a small chin, generous lips, small upturned nose, and flattened nose bridge, and puffiness under the eyes, along with a low birth weight, trouble breastfeeding, severe gag reflex, colic or irritability in the night, low muscle tone and general failure to thrive. Colic is thought to be brought on by higher than normal levels of calcium circulating in the blood, known as hypercalcaemia. Specific congenital heart defects are often detected at the baby’s first visit to the pediatrician, which assists in leading to the initial diagnosis of Williams Syndrome. When the characteristics of Williams Syndrome are recognized, referral to a clinical geneticist for further diagnostic evaluation would follow.
|
|

|
Other Indicators |

|

|

|
Feeding difficulties tend to resolve as the children get older.
Many infants with Williams syndrome have an extended period of colic or irritability. This typically lasts from 4 to 10 months of age, then resolves.. Abnormal sleep patterns with delayed acquisition of sleeping through the night may be associated with the colic.
Slightly small, widely spaced teeth are common in children with Williams syndrome. They also may have a variety of abnormalities of occlusion (bite), tooth shape or appearance. Most of these dental changes are readily amenable to orthodontic correction.
There is a slightly increased frequency of problems with kidney structure and/or function.
Inguinal (groin) and umbilical hernias are more common in Williams syndrome than in the general population.
Children with Williams syndrome often have more sensitive hearing than other children; certain frequencies or noise levels can be painful and/or startling to the individual. This condition often improves with age.
Young children with Williams syndrome often have low muscle tone and joint laxity. As the children get older, joint stiffness (contractures) may develop. Physical therapy is very helpful in improving muscle tone, strength and joint range of motion.
Most people with Williams syndrome will have mild to severe learning disabilities and cognitive challenges. Young children with Williams syndrome often experience developmental delays. Milestones such as walking, talking and toilet training are often achieved somewhat later than is considered normal. Distractibility is a common problem in mid-childhood, which can improve as the children get older.
Older children and adults with Williams syndrome often demonstrate intellectual "strengths and weaknesses." There are some intellectual areas (such as speech, long term memory, and social skills) in which performance is quite strong, while other intellectual areas (such as fine motor and spatial relations) show significant weakness.
Many infants with Williams syndrome have an extended period of colic or irritability. This typically lasts from 4 to 10 months of age, then resolves.. Abnormal sleep patterns with delayed acquisition of sleeping through the night may be associated with the colic.
Slightly small, widely spaced teeth are common in children with Williams syndrome. They also may have a variety of abnormalities of occlusion (bite), tooth shape or appearance. Most of these dental changes are readily amenable to orthodontic correction.
There is a slightly increased frequency of problems with kidney structure and/or function.
Inguinal (groin) and umbilical hernias are more common in Williams syndrome than in the general population.
Children with Williams syndrome often have more sensitive hearing than other children; certain frequencies or noise levels can be painful and/or startling to the individual. This condition often improves with age.
Young children with Williams syndrome often have low muscle tone and joint laxity. As the children get older, joint stiffness (contractures) may develop. Physical therapy is very helpful in improving muscle tone, strength and joint range of motion.
Most people with Williams syndrome will have mild to severe learning disabilities and cognitive challenges. Young children with Williams syndrome often experience developmental delays. Milestones such as walking, talking and toilet training are often achieved somewhat later than is considered normal. Distractibility is a common problem in mid-childhood, which can improve as the children get older.
Older children and adults with Williams syndrome often demonstrate intellectual "strengths and weaknesses." There are some intellectual areas (such as speech, long term memory, and social skills) in which performance is quite strong, while other intellectual areas (such as fine motor and spatial relations) show significant weakness.

|
References |
Better Health Channel. (2015) Symptoms of Williams Syndrome.
Retrieved 24th July 2015, from http://www.betterhealth.vic.gov.au/bhcv2/bhcarticles.nsf/pages/williams_syndrome
Grimm, T., & Wesselhoeft, H. (1980). The genetic aspects of Williams-Beuren syndrome and the isolated form of the supravalvular aortic stenosis. Investigation of 128 families. Z. Kardiol, 69, 168-172.
Herndon, J. (2012). Healthline. Williams Syndrome. Retrieved 23rd July 2015, from http://www.healthline.com/health/williams-syndrome#Overview1
Martens, M., Wilson, S., & Reutens, D. (2008). Research Review: Williams syndrome: a critical review of the cognitive, behavioral, and neuroanatomical phenotype. J Child Psychol & Psychiat, 49(6), 576-608. doi:10.1111/j.1469-7610.2008.01887.x
Stromme, P., Bjomstad, P., & Ramstad, K. (2002). Prevalence Estimation of Williams Syndrome. Journal Of Child Neurology, 17(4), 269-271. doi:10.1177/088307380201700406
Raisingchildren.net.au The Australian Parenting Website. (2014) Williams Syndrome. Retrieved 24th July 2015, from http://raisingchildren.net.au/articles/williams_syndrome.html
Williams-syndrome.org,. (2014). Understanding Williams Syndrome. Retrieved 22nd July, 2015 from http://understandingwilliamssyndrome.blogspot.com/p/growth-and-diet.html
Williams-syndrome.org,. (2015). What is Williams Syndrome? | Williams Syndrome Association. Retrieved 20 July 2015, from https://williams-syndrome.org/what-is-williams-syndrome
Retrieved 24th July 2015, from http://www.betterhealth.vic.gov.au/bhcv2/bhcarticles.nsf/pages/williams_syndrome
Grimm, T., & Wesselhoeft, H. (1980). The genetic aspects of Williams-Beuren syndrome and the isolated form of the supravalvular aortic stenosis. Investigation of 128 families. Z. Kardiol, 69, 168-172.
Herndon, J. (2012). Healthline. Williams Syndrome. Retrieved 23rd July 2015, from http://www.healthline.com/health/williams-syndrome#Overview1
Martens, M., Wilson, S., & Reutens, D. (2008). Research Review: Williams syndrome: a critical review of the cognitive, behavioral, and neuroanatomical phenotype. J Child Psychol & Psychiat, 49(6), 576-608. doi:10.1111/j.1469-7610.2008.01887.x
Stromme, P., Bjomstad, P., & Ramstad, K. (2002). Prevalence Estimation of Williams Syndrome. Journal Of Child Neurology, 17(4), 269-271. doi:10.1177/088307380201700406
Raisingchildren.net.au The Australian Parenting Website. (2014) Williams Syndrome. Retrieved 24th July 2015, from http://raisingchildren.net.au/articles/williams_syndrome.html
Williams-syndrome.org,. (2014). Understanding Williams Syndrome. Retrieved 22nd July, 2015 from http://understandingwilliamssyndrome.blogspot.com/p/growth-and-diet.html
Williams-syndrome.org,. (2015). What is Williams Syndrome? | Williams Syndrome Association. Retrieved 20 July 2015, from https://williams-syndrome.org/what-is-williams-syndrome
Home > Terminology > Characteristics > Causes,Diagnosis, Treatment > Prevalence & Early Warning Signs
Tips for Teachers > Classroom Management > Writing & Reading > Mathematics > Music
Tips for Teachers > Classroom Management > Writing & Reading > Mathematics > Music
Last modified: 30th July 2015
